The FDA launched its first real-time, AI-driven clinical trial pilot in May 2026. FDA Commissioner Marty Makary announced the program; FDA Chief AI Officer Jeremy Walsh said it could potentially cut 20, 30, or 40 percent of overall clinical trial time by streaming a direct data feed from live trials into cloud infrastructure for continuous monitoring instead of periodic batch reviews. AstraZeneca and Amgen ran the first trials. A public Request for Information closed May 29, 2026, with a pilot expansion decision expected during summer 2026. This is a structured exploration of AI inside the drug-approval pipeline — not a blanket approval of AI in regulatory decisions.
The Big Picture: A Regulator Rebuilds Its Own Plumbing
For decades the structural rhythm of drug approval has been periodic and retrospective. Sponsors run a trial, lock the database, compile the dataset, and submit it. Reviewers then analyze a finished snapshot after the fact. The calendar cost of that batch model is enormous — not because any single step is slow, but because the process is a sequence of waits.
The FDA's May 2026 pilot attacks that rhythm directly. Instead of reviewing a completed dataset, FDA regulators receive a direct data feed from a live clinical trial and observe patient outcomes — fever onset, tumor shrinkage — as events occur, through cloud infrastructure. The shift is not "AI reads the application faster." It is "the regulator watches the trial happen." That is a different category of change.
Commissioner Marty Makary announced the pilot at FDA headquarters in Silver Spring, Maryland. The driving force, credited publicly, is FDA Chief AI Officer Jeremy Walsh — a title that itself signals how seriously the agency is treating AI infrastructure as an executive function rather than a distributed side project.
The Pilot Mechanics: Cloud + AI as Continuous Monitoring
The technical core is deceptively simple to describe and hard to operate: a continuous, validated stream of trial data from sponsor to regulator. AI sits on top of that stream to surface signals; cloud infrastructure carries and stores the feed at scale.
From Batch Snapshots to Live Feeds
In the traditional model, the unit of regulatory work is a frozen dataset. In the pilot model, the unit is a stream. That sounds like a plumbing detail, but it changes the economics of elapsed time: a regulator who is already watching does not need a multi-month ramp-up to understand a dataset that lands all at once.
Who Is Running It First
AstraZeneca and Amgen are the two pharmaceutical companies conducting the initial trials under the system. The choice is not incidental. Both are large-cap, late-stage-heavy organizations with the data volume and infrastructure maturity to stress-test continuous monitoring without the pilot collapsing under operational friction.
The AI Layer, Specifically
The AI component is best understood as signal detection over a live feed — flagging outcomes worth a human regulator's attention as they arrive, rather than waiting for a sponsor to compile and narrate them months later. The human reviewer remains the decision-maker. This is an important boundary to state plainly because the headline framing of "FDA adopts AI" can imply autonomy that the pilot does not grant.
Why the Architecture Choice Matters
Cloud plus AI is not an arbitrary stack. A continuous feed is only useful if it is durable, queryable, and auditable at the moment a regulator looks at it — not reconstructed later from logs. Cloud infrastructure provides the elasticity to absorb variable trial data volumes; the AI layer provides the triage that makes a live stream legible instead of overwhelming. Strip either component and the model degrades back toward batch review. The pairing is the point, which is why the agency frames it as "AI plus cloud computing" rather than an AI feature bolted onto existing systems.
The 20-40 Percent Question: What Walsh Actually Said
The number drawing the most attention is Jeremy Walsh's estimate that the approach could reduce "20, 30, 40% of overall clinical trial time." It is worth being precise about what that claim is and is not.
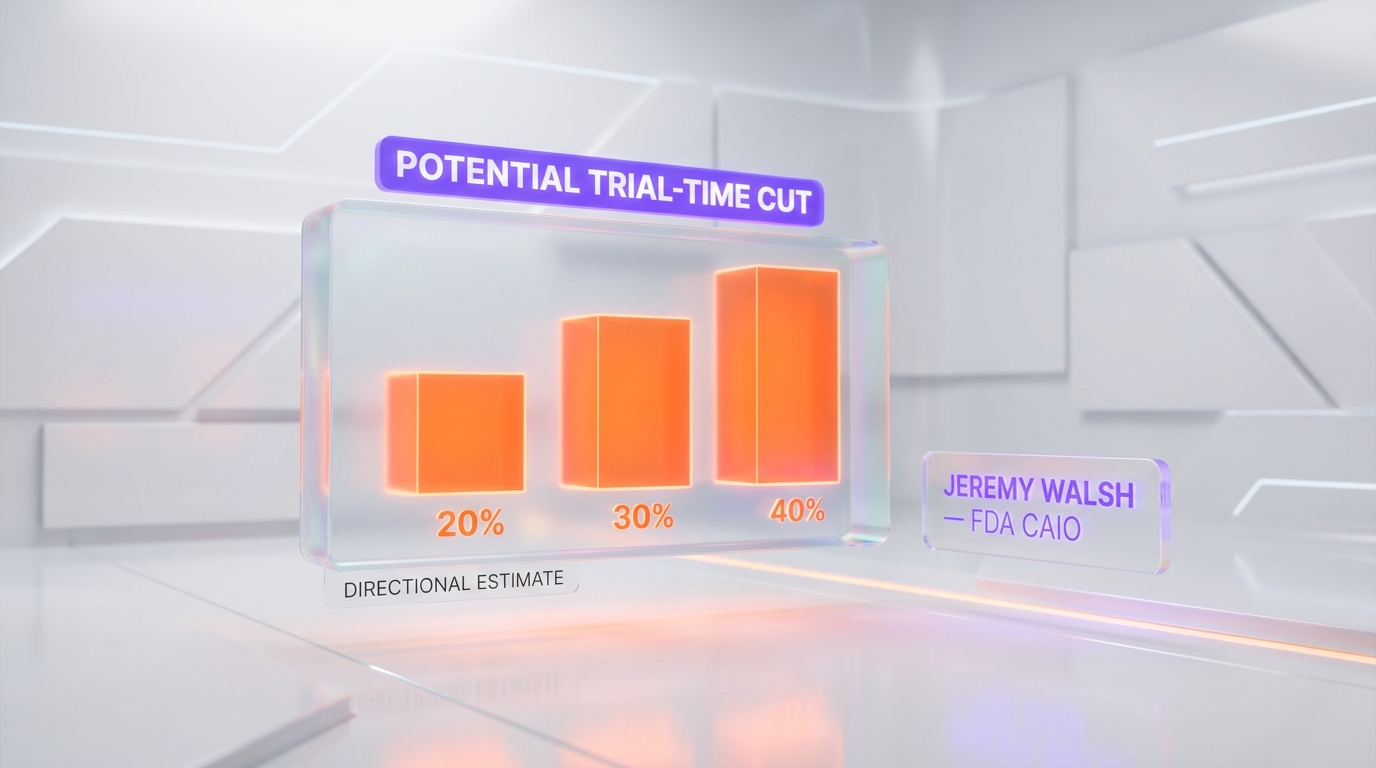
It Is a Directional Estimate, Not a Result
Walsh framed the figure as potential, attached to a pilot, and explicitly conditioned on not compromising safety. It describes the upper-bound opportunity of continuous monitoring if results hold across more programs — not a measured reduction already achieved in two trials. Treating it as a delivered metric would be exactly the kind of overstatement worth resisting.
Why the Range Is Plausible Structurally
Even as an estimate, the range is structurally coherent. Much of a trial's elapsed calendar time is not the science — it is the gaps: database lock, compilation, submission queues, review ramp-up. Continuous monitoring compresses the gaps, not the biology. That is why a 20 to 40 percent elapsed-time reduction is internally consistent even though it would not make any individual patient's treatment shorter.
What It Does Not Mean
It does not mean drugs reach patients 40 percent sooner in 2026. It does not mean Phase 3 endpoints are reached faster. And it does not mean the full regulatory timeline — including manufacturing review and post-market commitments — collapses by the same proportion. The figure is about trial-time elapsed waste, which is a real and large target, but a specific one.
The RFI Timeline: How a Pilot Becomes a Process
The single most important governance detail is that this is structured through a Request for Information, not announced as a finished policy.
RFI Closed May 29, 2026
The FDA released a public RFI soliciting input on how AI-enabled technologies could improve efficiency in early-phase clinical trials. Responses were due May 29, 2026. That deadline is the formal mechanism converting a two-company experiment into an evidence-gathering process with documented industry and public input.
Summer 2026: The Expansion Decision
Results from the initial pilot, combined with RFI input, could shape an expansion of the program during summer 2026. The decision point matters more than the announcement: a pilot that does not expand is a press release; a pilot that expands with refined selection criteria is a structural change to how trials are monitored.
Why the Sequencing Is the Real Signal
Pilot, then RFI, then expansion decision is a deliberately conservative sequence. It lets the agency claim momentum while keeping an exit. For anyone modeling the impact, the honest read is: the structural intent is clear, but the magnitude is unproven until the expansion decision and its criteria are public.
The FDA's Wider AI Adoption Arc
The trial pilot is the externally visible tip of a larger internal modernization. The FDA consolidated 40 separate application intake systems into one and reduced its monitoring and reporting systems, a change projected to save at least $120 million annually. The agency also reported over 80 percent generative AI adoption among employees.
This context reframes the pilot. It is not a regulator dabbling in AI on the trial side while everything else stays manual. It is a regulator rebuilding its own data infrastructure end to end, of which continuous trial monitoring is one externally facing component. The internal consolidation is arguably the harder, less glamorous, and more durable part of the story.
The sequencing also tells you something about institutional confidence. An agency that had not already consolidated 40 intake systems and driven generative AI adoption past 80 percent internally would have little operational basis to attempt continuous external trial monitoring. The pilot is downstream of an internal capability the agency built first. That ordering — internal infrastructure before external program — is the same pattern mature technology organizations follow, and it is a reason to take the pilot's structural intent seriously even while staying skeptical about the magnitude.
It also changes who the relevant decision-makers are. When AI infrastructure sits with a dedicated Chief AI Officer function rather than being scattered across program offices, decisions about continuous monitoring, vendor requirements, and expansion criteria are made coherently rather than per-division. That centralization is a quiet but meaningful governance signal: it means the pilot is being run as infrastructure strategy, not as a one-off experiment owned by whichever office happened to sponsor it.
Implications for Pharma: A New Infrastructure Expectation
If FDA-grade continuous monitoring becomes the expected mode, the burden does not sit only with the regulator. Sponsors and contract research organizations need compatible, validated, real-time-capable infrastructure on their side of the feed.
That advantages organizations that already operate at that maturity. AstraZeneca and Amgen are in the pilot precisely because they can. Smaller biotechs face a real question: does continuous monitoring become a competitive speed advantage that compounds the existing capital gap between large and small sponsors? This is one of the substantive risks the RFI process exists to surface — not a reason to halt, but a reason to design selection criteria carefully.
For context on how the largest pharma players are already wiring AI across their value chains, the Novo Nordisk and OpenAI six-domain integration is a useful adjacent reference point — including its explicit clinical-trials workstream. The FDA pilot and that partnership are two ends of the same arc: sponsors adopting AI internally, and the regulator adopting AI to watch the output.
Implications for AI Infrastructure: Regulatory-Grade Compute
A government regulator streaming live drug-trial data is one of the most demanding possible workloads: it must be auditable, tamper-evident, validated to GxP standards, highly available, and access-controlled at federal scale. That is a specific and lucrative category of demand for cloud and AI infrastructure providers.
The market read is structural. The scale of compute being assembled by frontier labs — for example, the buildout described in our analysis of Anthropic's gigawatt-scale compute empire — is the supply side of an economy where even regulators now run continuous AI pipelines. Demand is not only commercial; it is becoming institutional and regulatory.
The same dynamic is visible in adjacent scientific tooling. Work on making AI protein design accessible to working biologists shows the upstream end of the pipeline — discovery — getting AI-native at the same time the downstream end — regulatory review — does. When both ends move together, the infrastructure expectation for the middle hardens fast.
The Regulation Angle: Government Operationalizing AI
There is a broader 2026 pattern worth naming explicitly. Governments are moving from regulating AI from the outside to operationalizing it inside core processes. The executive branch's posture on AI is itself in motion — see our coverage of the White House AI pre-release review executive order — and the FDA pilot is the same trend expressed inside an agency: AI is no longer only the thing being governed; it is increasingly the infrastructure the government runs.
That distinction is the strategic core of this story. A pre-release review order treats AI as an object of oversight. A continuous-monitoring trial pilot treats AI as operational plumbing for oversight itself. Both are happening in the same year, in the same government, pointing the same direction.
How It Compares: Tools Behind the Shift
The pilot is vendor-neutral in its public framing, but the capability class it depends on is well represented in the current frontier model field. General-purpose reasoning systems such as Claude and Gemini 3.1 Pro illustrate the kind of long-context, structured-data reasoning that signal detection over a live trial feed would draw on. The point is not that any specific model is in the pilot — it is that the underlying capability is now broadly available, which is exactly why a regulator can attempt this in 2026 rather than 2030.
What Would Prove This Overhyped
To keep the analysis honest, here are the signals that would deflate the ambitious framing. First: the summer 2026 expansion decision arrives with vague criteria or quietly slips, indicating the pilot did not produce convincing evidence. Second: continuous monitoring delivers single-digit elapsed-time gains rather than anything near the 20 to 40 percent envelope. Third: the infrastructure burden proves so heavy that only the largest sponsors can comply, narrowing the program into a big-pharma-only mechanism rather than an industry-wide one.
None of those outcomes would mean the pilot failed outright. But any of them would convert the story from "the regulator restructured trial monitoring" to "the regulator ran another modernization pilot." The honest position today is that the structural intent is unambiguous and the magnitude is unproven until summer 2026.
Our Verdict
This is one of the more consequential AI-in-government developments of 2026 precisely because it is structural rather than rhetorical. The mechanism — continuous monitoring replacing batch review — targets the real source of trial-time waste: the gaps, not the science. The 20 to 40 percent estimate is directionally credible as an opportunity ceiling even though it is not a delivered result. The RFI sequencing is conservative in the right way, keeping the change evidence-gated.
The strategic takeaway: the US regulator is adopting AI as operational infrastructure inside the drug-approval pipeline, not merely regulating AI from the outside. Watch the summer 2026 expansion decision and its selection criteria — that, not the May announcement, is the moment this becomes either a durable structural shift or another well-intentioned pilot.
Editorial note: ThePlanetTools.ai has no affiliate relationship with the FDA, AstraZeneca, Amgen, or any vendor referenced in this analysis. This is independent editorial coverage based on public reporting, including Nextgov/Government Executive, and FDA public communications. Nextgov coverage was a primary source for the pilot details, RFI deadline, and the Walsh estimate.
Frequently Asked Questions
What did the FDA announce about real-time AI clinical trials in 2026?
FDA Commissioner Marty Makary announced a pilot that uses AI plus cloud computing to monitor clinical trial data continuously, replacing the traditional model of periodic batch reviews. A direct data feed streams patient outcomes — such as fever development or tumor shrinkage — to FDA regulators in near real time. AstraZeneca and Amgen are running the first trials under the system. The agency also released a public Request for Information on AI-enabled early-phase trial efficiency, with responses due May 29, 2026.
How much could AI cut clinical trial duration according to the FDA?
FDA Chief AI Officer Jeremy Walsh, credited as the driving force behind the initiative, said the approach could potentially reduce 20, 30, or 40 percent of overall clinical trial time. He emphasized that safety would not be compromised to achieve those gains. This is a directional estimate tied to a pilot, not a guaranteed outcome — the figure describes the upper end of what continuous monitoring might unlock if results hold across more programs.
Is the FDA approving AI for drug approval decisions?
No. This is a structured exploration, not a blanket approval of AI in regulatory decision-making. The FDA opened a Request for Information to gather public and industry input, ran an initial pilot with two pharma companies, and signaled that results could shape an expansion during summer 2026. AI is being used to observe trial data continuously; human regulators still make the approval calls. Framing this as "the FDA approves AI" overstates what has actually happened.
When was the FDA RFI deadline and what comes next?
The FDA Request for Information on AI-enabled technologies for early-phase clinical trial efficiency had a response deadline of May 29, 2026. Input collected through that window feeds into how the agency refines selection criteria and decides on an expansion of the pilot program during summer 2026. The RFI is the formal mechanism that turns a two-company pilot into a structured, evidence-gathering process rather than an ad hoc experiment.
Which pharma companies are in the FDA real-time AI trial pilot?
AstraZeneca and Amgen are the two pharmaceutical companies conducting the initial clinical trials using the real-time data feed system. Their participation matters because both are large-cap, late-stage-heavy organizations whose trial data volumes are substantial enough to stress-test continuous monitoring infrastructure. The pilot expansion decision in summer 2026 will likely determine whether additional sponsors join.
How does continuous monitoring differ from traditional FDA trial review?
Traditional review is periodic and retrospective: sponsors compile data, submit it in batches, and FDA reviewers analyze snapshots after the fact. Continuous monitoring streams a direct data feed from the trial into cloud infrastructure so regulators can observe patient outcomes as events occur. The structural shift is from reviewing a finished dataset to watching a live one — which is what compresses elapsed calendar time without removing safety checkpoints.
What is the role of Jeremy Walsh, the FDA Chief AI Officer?
Jeremy Walsh is the FDA Chief AI Officer and was credited as the driving force behind the real-time clinical trial pilot. He is the source of the 20, 30, 40 percent trial-time reduction estimate and the public voice tying the pilot to the agency’s broader AI adoption. His role signals that AI infrastructure decisions inside the FDA now sit with a dedicated executive function rather than being distributed across program offices.
How does this connect to the FDA’s wider AI adoption push?
The pilot sits inside a larger modernization arc. The FDA consolidated 40 separate application intake systems into one and reduced monitoring and reporting systems, projected to save at least $120 million annually. The agency also reported over 80 percent generative AI adoption among employees. Real-time trial monitoring is the externally facing piece of an internal infrastructure overhaul — the regulator is rebuilding its own data plumbing, not just asking sponsors to change.
What does this mean for AI infrastructure and cloud vendors?
A regulator running continuous data feeds from live drug trials needs validated, auditable, high-availability cloud infrastructure with strict data governance. That creates demand for regulatory-grade compute, secure pipelines, and observability tooling at federal scale. It also sets a reference architecture: if FDA-grade continuous monitoring becomes standard, sponsors and CROs will need compatible infrastructure on their side, expanding the addressable market well beyond the two pilot companies.
What are the main risks of real-time AI trial monitoring?
Three structural risks dominate: data integrity (a live feed must be tamper-evident and validated to GxP standards), over-interpretation (watching interim data in real time raises the temptation to act on noise before statistical significance), and unequal access (large sponsors like AstraZeneca and Amgen can build compatible infrastructure faster than smaller biotechs, potentially widening the speed gap). None of these are reasons not to proceed — they are the items the RFI process exists to surface and constrain.
Could this speed up drug approvals for patients in 2026?
Not within 2026. This is a pilot whose expansion decision comes in summer 2026, and the 20 to 40 percent figure describes elapsed trial time, not the full approval timeline. Even an optimistic reading means measurable patient-facing acceleration is a 2027-and-beyond outcome, contingent on the pilot expanding, the infrastructure validating cleanly, and sponsors adopting compatible systems. The near-term effect is structural groundwork, not faster drugs this year.
How does this fit the broader 2026 AI-in-regulation trend?
It is part of a visible 2026 pattern of governments operationalizing AI inside core processes rather than only regulating it from the outside. Alongside executive-branch moves on AI pre-release review and pharma’s own AI integrations with frontier labs, the FDA pilot shows the US regulatory apparatus adopting AI in the approval pipeline itself. The strategic read: AI is moving from "thing being regulated" to "infrastructure the regulator runs."